Irritable Bowel Syndrome (IBS)
- Posted on
- By Gabriela Mancilla Valdez, CHN, RA
- Posted in Constipation, Diarrhea, IBS, Postbiotic, Prebiotic, Probiotic

In this blog post, we dive into the condition Irritable Bowel Syndrome (IBS). We discuss its causes, symptoms, types, and diagnostic criteria, as well as how to support it with diet, lifestyle, and supplementation.
In this blog post, we are going to dive into Irritable Bowel Syndrome (IBS), the most commonly diagnosed GI disorder constituting 30-50% of all referrals to gastroenterologists. It is highly likely there are more people that have IBS than people that know what IBS is. 10-15% of people in the western world are affected by IBS, but it is likely largely undiagnosed. Out of those diagnosed with IBS, women predominate at a 2:1 ratio.
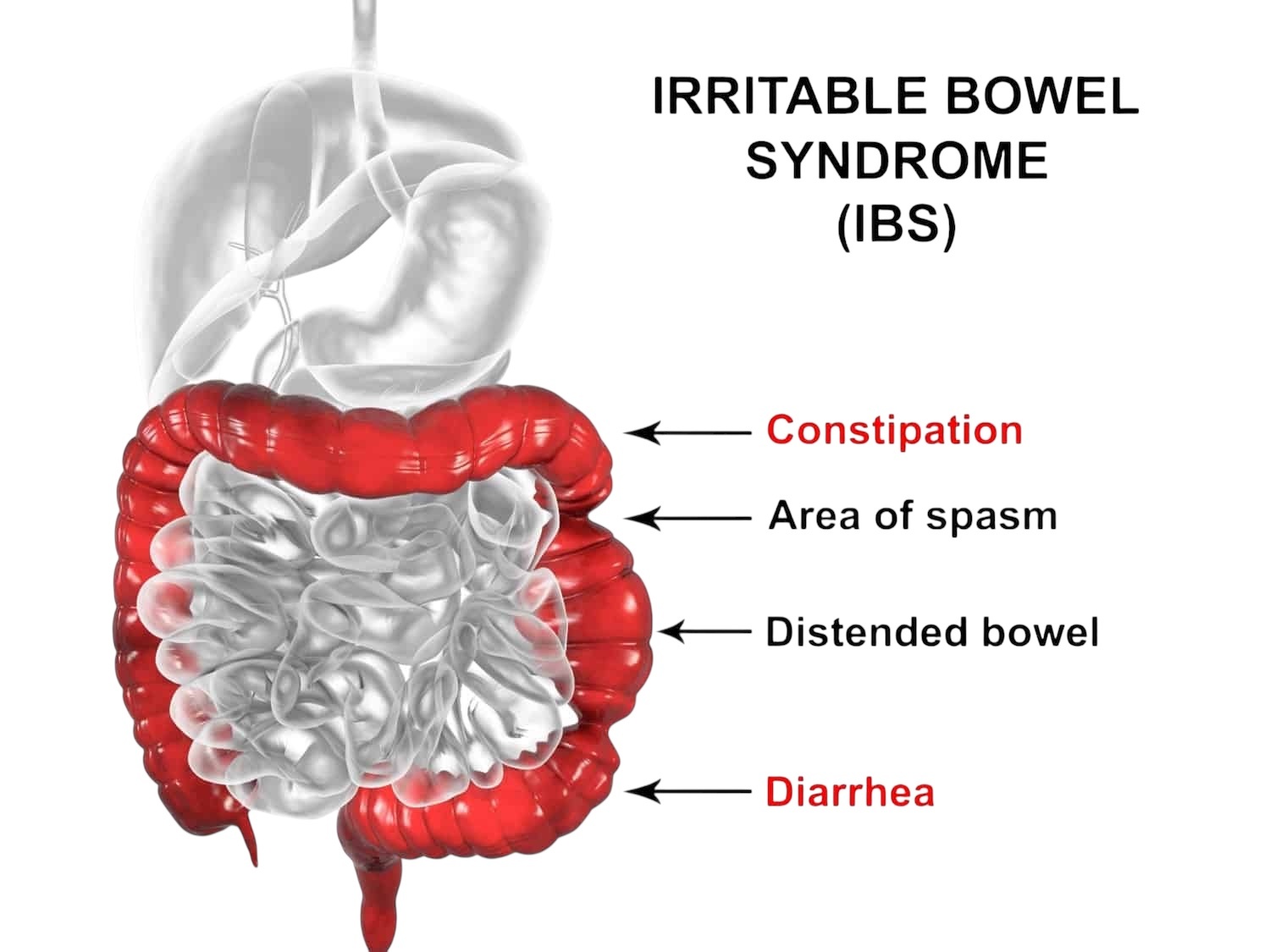
IBS is a functional bowel disorder characterized by intermittent and chronic abdominal pain associated with a change in bowel movements; either constipation, diarrhea, or both. Although there is no cure to IBS, there are therapeutic options to alleviate symptoms of IBS. In this blog, we will discuss how IBS develops, its signs and symptoms, treatment and therapeutic options, and dietary recommendations.
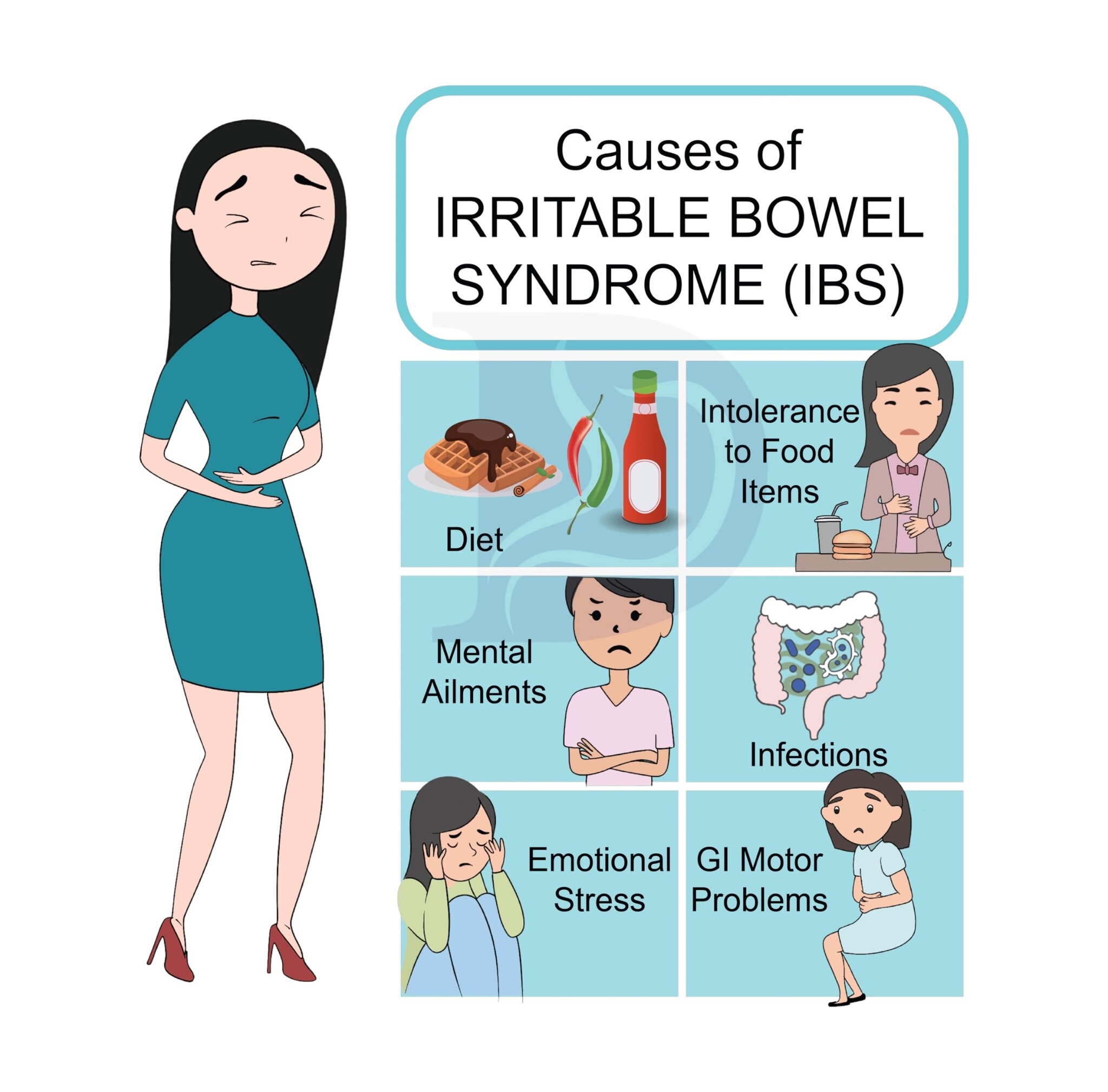
Although the etiology of IBS is unknown, there are issues that are known to contribute to IBS. The onset of IBS is in young adulthood, normally in the 20s. There is no organic cause, but IBS may be due to problems with regulation of gastrointestinal muscular activity, and is thus considered to be a functional bowel disorder. It is also known that the causes are the result of a mixture of digestive secretions, bacterial flora, and dietary factors.
It is also hypothesized that food allergies are a possible contributing factor to IBS because approximately two out of three IBS patients have at least one food intolerance and some have multiple. The most common allergens are dairy products (40-44%) and grains (40-60%); the most frequently reported symptoms are due to foods rich in carbohydrates, fatty food, alcohol, coffee, and hot spices.
The factors that are known to contribute to IBS include gastrointestinal motility disturbances, visceral hypersensitivity and altered perception, which may result from a remodeling of neural pathways in gut-brain access, psychiatric symptoms including anxiety and depression, intestinal inflammation as seen by increased lymphocytes and mast cells, fecal microbiome disruptions due to bacterial overgrowth, and post-infectious E. Coli and Campylobacter bacteria. Some diseases that can cause IBS or make IBS worse include Fibromyalgia, Chronic Fatigue Syndrome, GERD, Major depressive disorder (MDD), and anxiety.
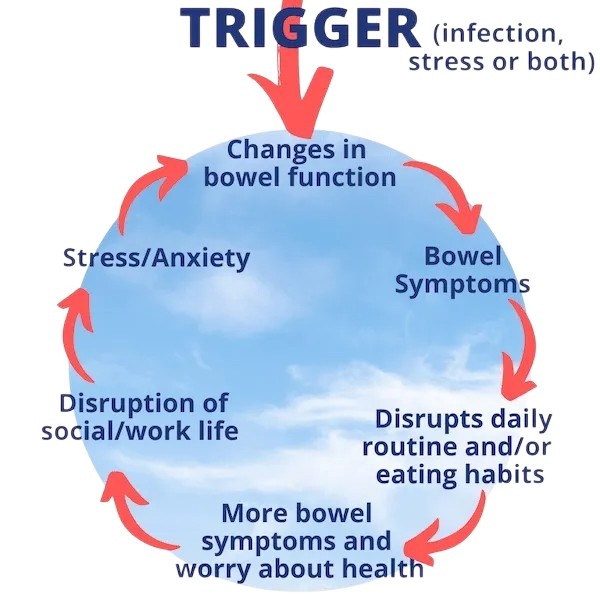
The signs and symptoms of IBS include symptoms associated with abdominal pain, indigestion, and elimination. The symptoms are often triggered by food or stress. The first main symptom of IBS is abdominal pain associated with defecation, which is a cramping pain of variable intensity and location. A second main symptom is a change in stool frequency and/or consistency, either diarrhea or constipation. With diarrhea, it most often occurs in the morning or after eating and is preceded by lower abdominal pain and a sense of urgency, possibly with tenesmus, which is having the feeling of needing to go to the bathroom yet you cannot go to the bathroom. With constipation, it is a pellet shaped stool and can also have a sensation of tenesmus. Other associated symptoms of IBS include straining, urgency, tenesmus, passage of mucus, bloating and abdominal distension, flatulence, nausea, anorexia, and varying degrees of anxiety and depression.
The diagnostic criteria is the Rome IV criteria, assessed using a bowel habit journal: symptoms at least one day per week in the past three months of abdominal discomfort associated with at least two of the following, relieved/related with defecation, change in stool frequency, or change in stool consistency.
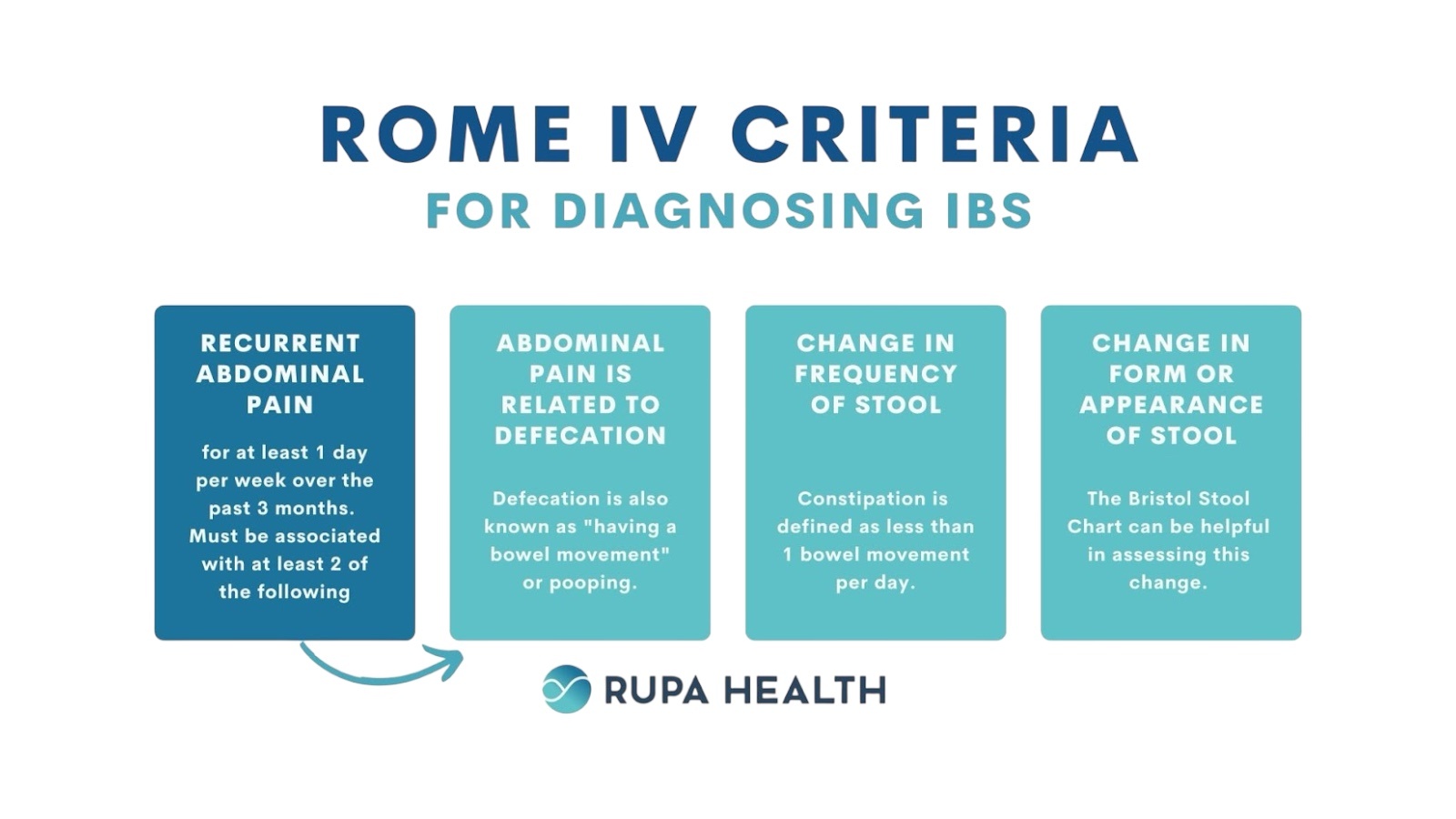
This criteria is used when other diseases that can mimic IBS are eliminated including cancer, diarrhea caused by infections, disturbed microflora due to antibiotic or antacid use, diverticular disease, IBD, intestinal candidiasis, lactose intolerance, laxative abuse, malabsorption diseases, mechanical causes like fecal impaction, metabolic disorders, or dietary factors interfering with digestion such as excessive consumption of tea, coffee, carbonated beverages, and simple sugars. It is also necessary to rule out red-flag symptoms including onset after age 50, anemia, fever, melena/hematochezia, nocturnal defecation, unexplained weight loss, and laboratory abnormalities. Symptoms that can support the diagnosis include change in frequency of more than three times a day for diarrhea or less than three times per week for constipation, more than ¼ of bowel movements changing in consistency, more than ¼ of bowel movements changing with sensation, more than ¼ bowel movements passing mucus, and sensation of bloating.
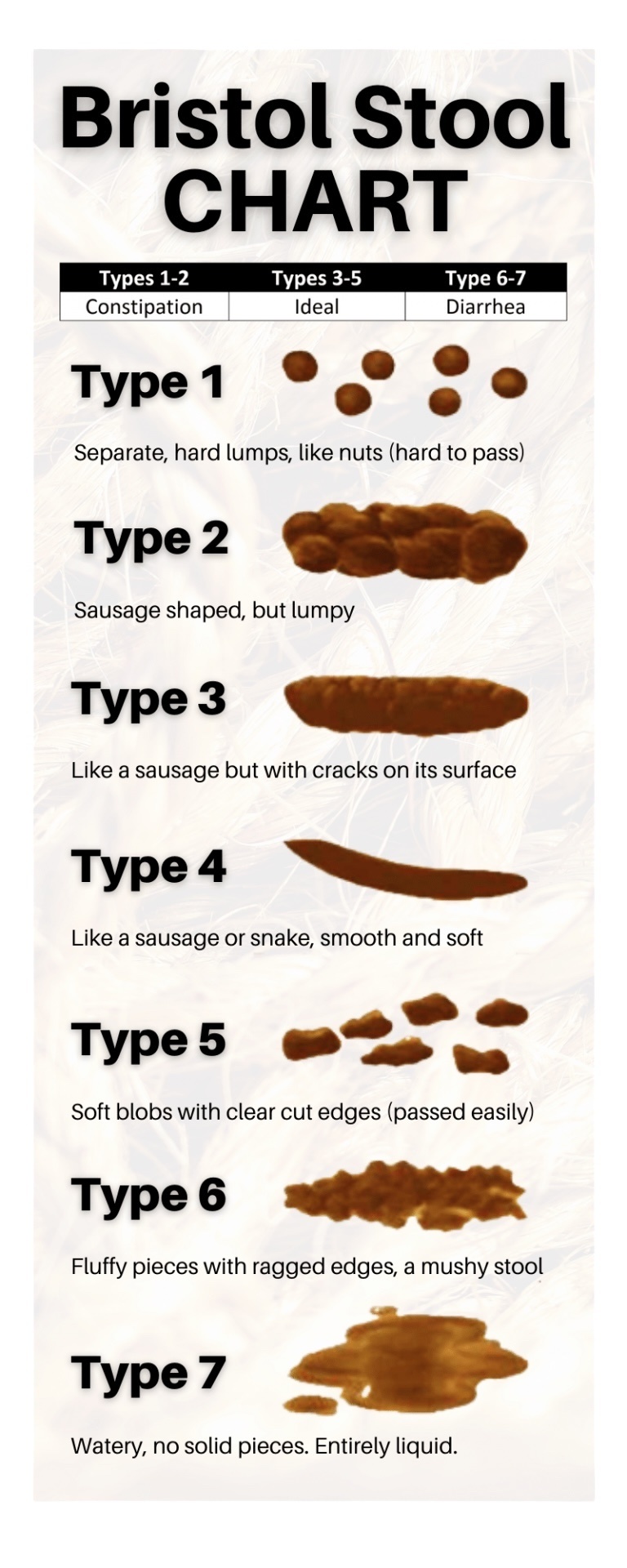
There are four types of IBS: IBS-D, IBS-C, IBS-M, and IBS unclassified. IBS with predominant diarrhea (IBS-D) is primarily diarrhea with more than 25% of bowel movements as Bristol types 6 and 7 and less than 25% of bowel movements as Bristol types 1 and 2. IBS with predominant constipation (IBS-C) is more than 25% of bowel movements as Bristol types 1 and 2 and less than 25% of bowel movements as Bristol types 6 and 7. IBS with mixed bowel habits (IBS-M) is alternating diarrhea and constipation with more than 25% of bowel movements as Bristol types 6 and 7 and more than 25% of bowel movements as Bristol types 1 and 2. IBS unclassified is a change in stool consistency that is insufficient to categorize.
There is no way to recover from IBS, so there is no “recovery”. Although there is no recovery, there may be changes over time. In the long term prognosis of IBS, symptoms appear to improve with increasing age with 80% of patients having improvement of symptoms over time. Additionally, the IBS subtype may change over time and patients with IBS have a normal life expectancy. The treatment consists of addressing the root cause of the symptoms.
The western medical treatment for IBS uses medication directed toward the dominant presenting symptoms. As opposed to the western treatment that focuses on drugs that primarily suppress symptoms, studies have shown that improving digestion sometimes resolves symptoms of IBS. In a study of IBS patients, 63% of the patients had GI symptoms related to meals especially those rich in carbohydrates, fatty foods, coffee, alcohol, and hot spices.
Another study hypothesized that since food ingestion, through mechanosensation and nutrient sensing, causes major changes in GI sensorimotor and secretory function, food processing may contribute to symptom generation in IBS. Digestion is hindered from the inhibition of GI motility. GI motility can be hindered by meals high in sugar and by stress. When a meal high in sugar is ingested, blood glucose levels rise too rapidly and peristalsis slows down. Studies have shown that meals high in refined sugar can contribute to IBS as well as SIBO by decreasing intestinal motility.
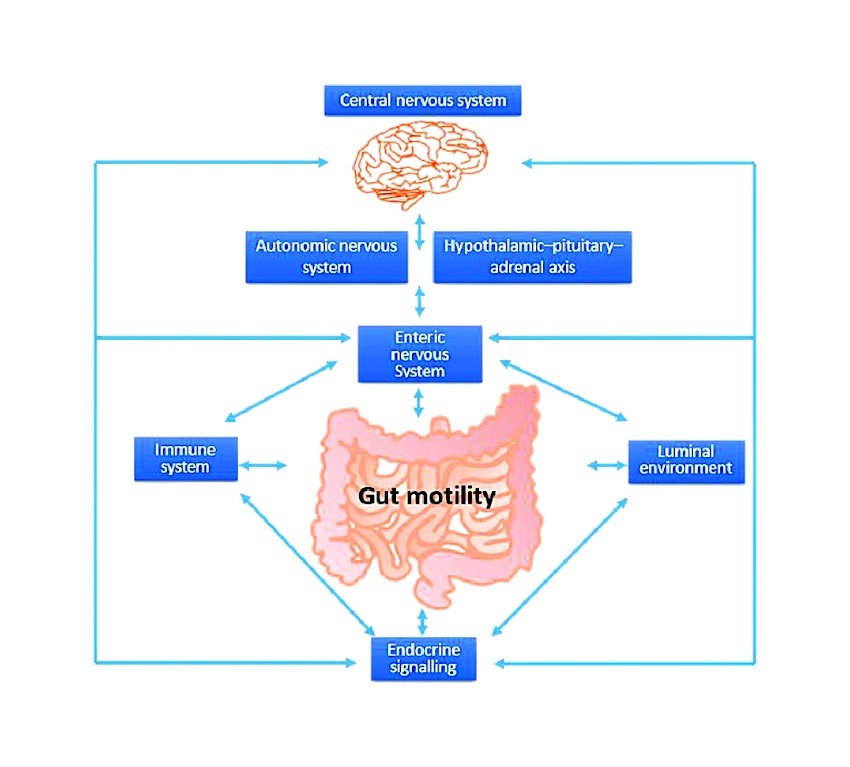
Stress has also been shown to increase intestinal motility in patients with IBS and people without IBS; it accounts for the increase in abdominal pain and irregular bowel functions in all people during times of stress.
Dietary recommendations to support IBS patients mainly focus on adding fiber, avoiding trigger foods, appropriate hydration, and elimination diets. IBS patients should aim for 30 grams of fiber a day. Bran and psyllium are two types of fiber recommended for IBS patients, however wheat bran is usually contraindicated because wheat and other grains are among the foods most commonly implicated in malabsorptive and allergic conditions and as discussed above, food allergy is a significant etiological factor in IBS. Thus, fiber should mainly come from fruit and vegetables.
Supplements can also be used to achieve fiber goals. Psyllium husks are a popular fiber supplement for IBS. Our recommended Psyllium Husk supplement is Organic Psyllium Husk Powder Metabolic Maintenance. Another supplement that has fiber from multiple sources including Psyllium Husks is Gastro-Fiber Standard Process. Some of our top fiber supplements include: OptiFiber Lean Xymogen. TruFiber Master Supplements and Fiber Formula Integrative Therapeutics.
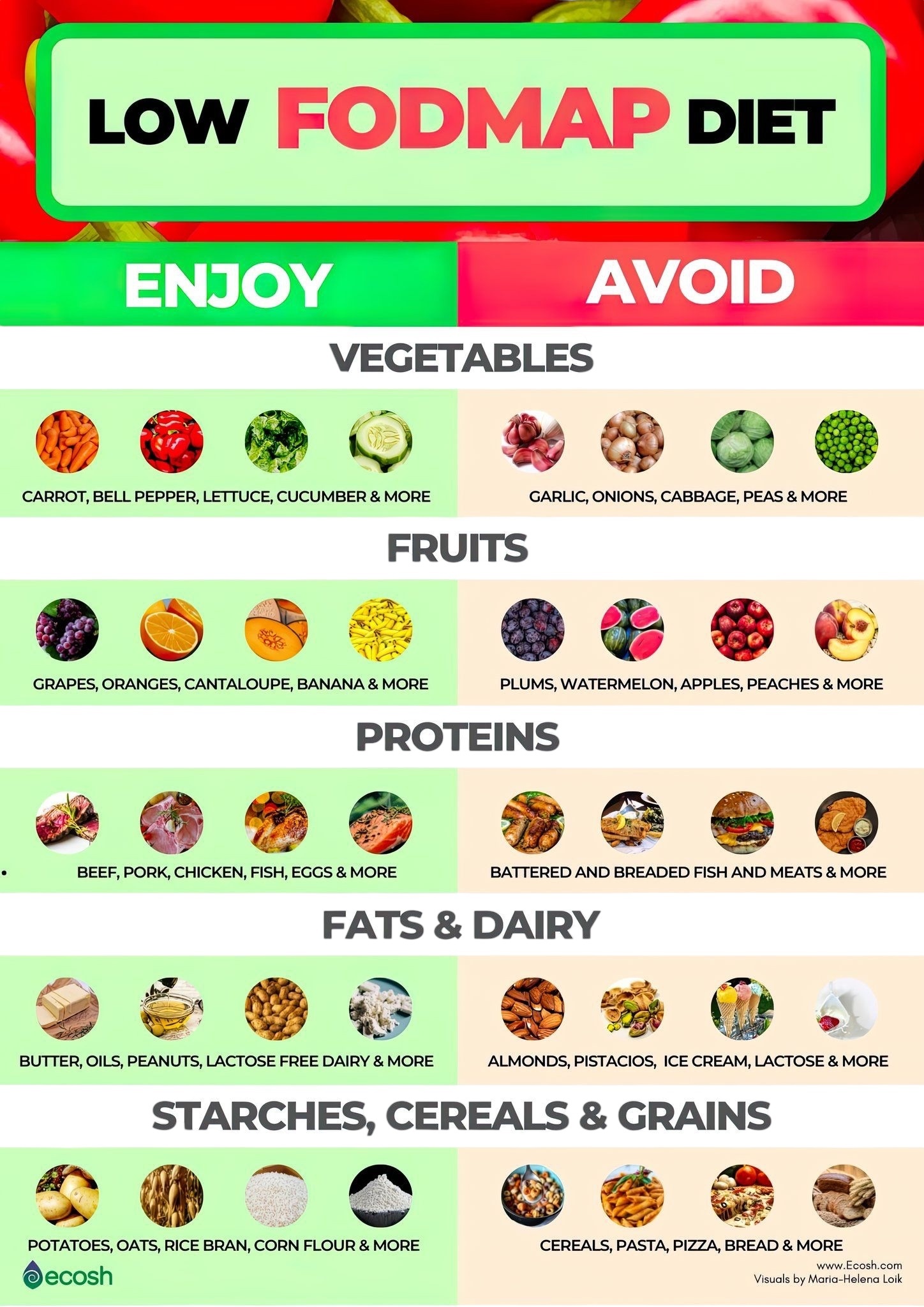
A low FODMAP diet is also recommended for IBS patients since food that is poorly absorbed in the small intestine is likely to be fermented by intestinal bacteria, which produces a large amount of gases causing abdominal bloating. In one study, 75% of patients saw a decrease in symptoms when they restricted FODMAP intake; a randomized placebo controlled rechallenge trial confirmed that this reduction of symptoms was due to the reduction of FODMAP intake.
Identifying food intolerances and then following a subsequent elimination diet has been shown to help IBS patients. In a 2006 study, 20 patients underwent food elimination diets based on the results of food and mold panels followed by a controlled food challenge. Significant improvements were seen in stool frequency and pain indicating that food elimination diets may be an effective treatment for IBS patients.
Patients with IBS should avoid lactose, gluten, and excess caffeine. They should also eliminate allergenic and intolerant foods, and refined sugars. It is important to have adequate hydration for those patients with IBS-C to prevent constipation. Meals should not be overly large, and eating should be slow and paced to avoid indigestion.
There are many supplements that can be used to address the symptoms and the problems with gastrointestinal motility in IBS. For a list of some of the recommended supplements for IBS click here.
Probiotics are one of the main supplements used in IBS since alterations in the gut microbiome can cause or exacerbate IBS symptoms. Randomized controlled clinical trials using probiotics have shown benefits of using probiotics for IBS, but they are not likely to resolve all symptoms. For a list of our probiotic options click here. For IBS, it is recommended to take spore forming probiotics at 4 billion CFUs. For a spore forming probiotic at this dosage, try Megaspore Biotic Microbiome Labs or Ortho Spore IG Ortho Molecular.

Studies have shown that Bifidobacterium infantis produced improvement in all IBS symptoms except stool frequency and consistency. A mixture of Lactobacillus rhamnosus GG, L. rhamnosus, Bifidobacterium breve, and Propionibacterium freudenreichii used for six months was shown to improve total symptom scores for abdominal pain, distension, flatulence, and bowel rumbling. For a probiotic containing Lactobacillus rhamnosus and Bifidobacterium breve, see ABx Support SFI. Additionally, Propionibacterium freudenreichiiis is abundant in cheese, specifically Swiss, so you can include cheese in your diet for that strain.
Enteric coated peppermint oil is another supplement that has shown to be effective with IBS. It inhibits GI smooth muscle action, improves rhythmic contractions of the intestinal tract, and relieves intestinal spasm. It has also been shown to be effective against Candida albicans, which can be an underlying factor in IBS. IBS patients using enteric coated peppermint oil have seen improvement in abdominal pain, abdominal distention, stool frequency, stomach rumbling, and flatulence. For enteric coated peppermint oil, we recommend IB Care BioClinic Naturals or Peppermint Oil G.I. Protocol for Life.
Ginger is another supplement that has shown to be effective against IBS. It may improve constipation by stimulating the activity of the migrating motor complex, which is the nerve and muscle complex that promotes peristalsis and elimination. In one study, treatment with 200 mg of ginger helped to increase the activity of the migrating motor complex; this is helpful in IBS because lack of activity of the migrating motor complex may contribute to SIBO, which is a causative factor in IBS. One of our recommended ginger supplements is Ultimate Ginger Complex Arcana.
Artichoke leaf can be helpful for improving digestive function by promoting bile production and can help relieve IBS symptoms. In one study, 640 mg of artichoke leaf extract taken three times daily almost completely eliminated abdominal pain, cramps, bloating, flatulence, and constipation in IBS patients. Our recommendation for artichoke is Artichoke Extract Jarrow. One clinical study looked at the combination of artichoke and ginger in treatment and found a significant improvement in nausea, bloating, epigastric fullness, and pain. A supplement that we offer including both ginger and artichoke is Motility Activator Integrative Therapeutics.

Digestive enzymes taken with meals can improve symptoms related to foods that commonly trigger IBS type symptoms, including lactose and beans. Additionally, since there may be mild Exocrine pancreatic insufficiency, undiagnosed food intolerances or sensitivities, or sensitivities to high FODMAP foods, digestive enzymes can help improve mealtime symptoms of IBS. For digestive enzymes tailored for digestion of beans, try Similase BV Integrative Therapeutics; for enzymes tailored to lactose digestion, try Gluten/Dairy Digest Pure or Similase GFCF Integrative Therapeutics. For a list of all of our digestive enzymes, click here. For more information on how digestive enzymes play a role in digestion, see the blog post: Digestion 101-Physio and Pathophysiology- Part II.
Melatonin can help IBS patients with symptom relief as well. One study in people with IBS and sleep disturbances showed that 3 mg of melatonin taken prior to bedtime for two weeks significantly decreased abdominal pain and rectal sensitivity and another study showed that the same dose reduced abdominal pain and bloating in women with IBS. For Melatonin in a 3mg dose, try Melatonin 3mg Pure or for a time release formula, try Melatonin Time Release 3mg Source Naturals.
Berberine is another supplement that may be useful for IBS. In animals, it helped reduce visceral hypersensitivity. It has shown to be effective for the treatment of diarrhea; in a study on patients with IBS-D, treatment with Berberine for eight weeks significantly reduced frequency of diarrhea, abdominal pain, and urgency with defection. It also improved scores of IBS symptoms, quality of life, depression, and anxiety. Some options for Berberine supplements are Berberine Thorne, Berberine Integrative Therapeutics, and Berberine Complex Integrative Therapeutics. For more information on Berberine, check out our Berberine Monograph.
Another aspect in the treatment of IBS is to control the psychological components, especially stress. Anxiety, fatigue, hostile feelings, depression, and sleep disturbances are reported by almost all patients with IBS and symptom severity and frequency tend to correlate with these psychological factors. In one study, anxiety was shown to be associated with a high degree of food related symptoms in IBS. Poor sleep quality also showed a rise in symptom severity in IBS patients.
Some herbal treatments for stress and anxiety in IBS include adaptogenic and nervine herbs. Some herbs to use include Bacopa, Holy Basil, and Ashwagandha. The adaptogenic properties of these herbs help to support the adrenals to mitigate stress; the nervine qualities of the herbs help to calm the mind to address stress and anxiety. Melatonin can be helpful in addressing the sleep disturbances of IBS patients as discussed above.
Some adaptogenic and nervine supplement options we recommend include Adaptocrine Apex: this formula contains holy basil and Ashwagandha as well as ingredients for digestive support which would be helpful in IBS. For Bacopa on its own, try Bacopa monnieri Pure or for a formula that includes Bacopa try Bacopa Plus drops Ayush Herbs or Bacopa Complex Standard Process.
There are a few alternative treatments that have shown to help improve symptoms of IBS including hypnosis, relaxation therapy, cognitive behavioral therapy, acupuncture, and exercise. In a study on IBS patients who still had symptoms despite previous treatment attempts, 12 weeks of weekly hypnotherapy sessions significantly improved IBS symptoms at three months compared with controls; the improvements seen at three months were also maintained at one year. In one study, IBS patients received a 10 session regimen of abbreviated progressive muscle relaxation with regular home practice and showed significant improvement compared to the control group with 50% of the relaxation group clinically improved at the end of the treatment.
Treatment with cognitive behavioral therapy was found to moderately to substantially improve IBS symptoms in almost 56% of individuals after two weeks. In two meta-analyses, acupuncture was found to be more effective than pharmaceutical treatment of IBS and to have the least severe side effects.
Light to moderate exercise has shown to be beneficial for IBS patients, but particularly intense exercise can be a contributing factor to IBS and should be avoided. In one study, patients who engaged in 20-60 minutes of moderate to vigorous physical activity 3-5 days per week experienced a marked improvement in quality of life and reduced IBS severity. Another study showed that thirty minutes of treadmill exercise three times a week for six weeks significantly improved IBS symptoms and improved quality of life compared to the no exercise control group. It has also been shown that walking regularly improves symptoms of IBS and it has a positive effect on mood.
In this post, we discussed the etiology, onset, symptoms, and potential therapeutic options and treatments for IBS. Although there is no cure for IBS, there are many natural treatments that studies have shown to be effective in symptom improvement of IBS. Every patient’s case is different, so it is good that there are so many options for treatment such that each patient can find a treatment that works for them.
References
Aguiar S, Borowski T. Neuropharmacological review of the nootropic herb Bacopa monnieri. Rejuvenation Res. Aug 2013;16(4):313-26. doi:10.1089/rej.2013.1431
Berkowitz, A. (2022). Clinical Pathophysiology made ridiculously simple: Edition 2. Medmaster.
Blanchard EB, Greene B, Scharff L, et al. Relaxation training as a treatment for irritable bowel syndrome. Biofeedback & Self Regulation 1993;18:125-132.
Brenner DM, Moeller MJ, Chey WD, Schoenfeld PS. The utility of probiotics in the treatment of irritable bowel syndrome: a systematic review. The American Journal of Gastroenterology 2009 Apr; 104(4): 1033-1049.
Deloose E, Janssen P, Depoortere I, Tack J. The migrating motor complex: control mechanisms and its role in health and disease. Nat Rev Gastroenterol Hepatol. Mar 27 2012;9(5):271-85. doi:10.1038/nrgastro.2012.57
Drisko J, Bischoff B, Hall M, McCallum R. Treating irritable bowel syndrome with a food elimination diet followed by food challenger and probiotics. Journal of the American College of Nutrition 2006 Dec; 25(6): 514-522.
Eswaran S, Tack J, Chey WD. Food: the forgotten factor in the irritable bowel syndrome. Gastroenterology Clinics of North America 2011 Mar;40(1): 141-162.
Fani M, Mostamand J, Fani M, Chitsaz N, Feizi A. The effect of aerobic exercises among women with mild and moderate irritable bowel syndrome: A pilot study. J Body Mov Ther. Jan 2019;23(1):161-165. doi:10.1016/j.jbmt.2018.02.003
Giacosa A, Guido D, Grassi M, et al. The Effect of Ginger (Zingiber officinalis) and Artichoke (Cynara cardunculus) Extract Supplementation on Functional Dyspepsia: A Randomised, Double-Blind, and Placebo-Controlled Clinical Trial. Evid Based Complement Alternat Med. 2015;2015:915087. doi:10.1155/2015/915087
Goldsmith G, Levin JS. Effect of sleep quality on symptoms of irritable bowel syndrome. Digestive Diseases and Sciences 1993;38:1809-1814.
JJ Medicine. (2019, Dec 18). Irritable Bowel Syndrome (IBS): Causes, Symptoms, Bristol Stool Chart, Types and Treatment [Video]. YouTube. https://www.youtube.com/watch?v=XaFYLNKebr8&t=1s
Johannesson E, Simrén M, Strid H, Bajor A, Sadik R. Physical activity improves symptoms in irritable bowel syndrome: a randomized controlled trial. The American journal of gastroenterology. May 2011;106(5):915-22. doi:10.1038/ajg.2010.480
Lackner JM, Jaccard J, Keefer L, et al. Improvement in Gastrointestinal Symptoms After Cognitive Behavior Therapy for Refractory Irritable Bowel Syndrome. Gastroenterology. Jul 2018;155(1):47-57. doi:10.1053/j.gastro.2018.03.063
Lindfors P, Unge P, Arvidsson P, et al. Effects of gut-directed hypnotherapy on IBS in different clinical settings-results from two randomized, controlled trials. The American journal of gastroenterology. Feb 2012;107(2):276-85. doi:10.1038/ajg.2011.340
Lu WZ, Gwee KA, Moochhalla S, Ho KY. Melatonin improves bowel symptoms in female patients with irritable bowel syndrome: a double-blind placebo-controlled study. Alimentary pharmacology & therapeutics. Nov 15 2005;22(10):927-34. doi:10.1111/j.1365-2036.2005.02673.x
Malik, Z. (2024, May). Irritable Bowel Syndrome (IBS). Merck Manual. https://www.merckmanuals.com/professional/gastrointestinal-disorders/irritable-bowel-syndrome-ibs/irritable-bowel-syndrome-ibs?query=irritable%20bowel%20syndrome%20(ibs)
Manheimer E, Wieland LS, Cheng K, et al. Acupuncture for irritable bowel syndrome: systematic review and meta-analysis. The American journal of gastroenterology. Jun 2012;107(6):835-47; quiz 848. doi:10.1038/ajg.2012.66
Murray, M.T. & Pizzorno, J. (2012). The Encyclopedia of Natural Medicine: Third Edition. Atria.
Nanda R, James R, Smith H, et al. Food intolerance and the irritable bowel syndrome. Gut 1989;30:1099-1104.
Narducci F, Snape WJ Jr, Battle WM, et al. Increased colonic motility during exposure to a stressful situation. Digestive Diseases and Sciences 1985:30:40-44.
Niedzielin K, Kordecki H. Birkenfeld B. A controlled double-blind, randomized study on the efficacy of Lactobacillus plantarum 299V in patients with irritable bowel syndrome. European Journal of Gastroenterology & Hepatology 2001;13: 1143-1147.
O’Mahony L, McCarthy J, Kelly P, et al. Lactobacillus and bifidobacterium in irritable bowel syndrome: symptom responses and relationship to cytokine profiles. Gastroenterology 2005 Mar; 128(3): 541-551.
Portincasa P, Bonfrate L, Scribano ML, et al. Curcumin and Fennel Essential Oil Improve Symptoms and Quality of Life in Patients with Irritable Bowel Syndrome. Journal of gastrointestinal and liver diseases : JGLD. Jun 2016;25(2):151-7. doi:10.15403/jgld.2014.1121.252.ccm
Russo A, Fraser R, Horowitz M. The effect of acute hyperglycemia on small intestinal motility in normal subjects. Diabetologia 1996;39:984-989.
Sandhaus, S. & Decker, C. (2024). Irritable Bowel Syndrome (IBS). Life Extension. https://www.lifeextension.com/protocols/gastrointestinal/irritable-bowel-syndrome
Shahabi L, Naliboff BD, Shapiro D. Self-regulation evaluation of therapeutic yoga and walking for patients with irritable bowel syndrome: a pilot study. Psychol Health Med. 2016;21(2):176-88. doi:10.1080/13548506.2015.1051557
Shepherd SJ, Gibson PR. Fructose malabsorption and symptoms of irritable bowel syndrome: guidelines for effective dietary management. Journal of the American Dietetic Association 2006;106:1631-1639.
Shepherd SJ, Parker FC, Muir JG, et al. Dietary triggers of abdominal symptoms in patients with irritable bowel syndrome: randomised, placebo-controlled evidence. Clinical Gastroenterology and Hepatology 2008;6:765-771.
Simren M. Mansson A, Langkilde AM, et al. Food-related gastrointestinal symptoms in the irritable bowel syndrome. Digestion 2001;63:108-115
Singh RH, Lallan S. Studies on the anti-anxiety effect of the medhya rasayana drug brahmi (Bacopa moniera Wettst), part 1. Journal of Research in Ayurveda and Siddha. 1981;1:138-148.
Song GH, Leng PH, Gwee KA, Moochhala SM, Ho KY. Melatonin improves abdominal pain in irritable bowel syndrome patients who have sleep disturbances: a randomised, double blind, placebo controlled study. Gut. Oct 2005;54(10):1402-7. doi:10.1136/gut.2004.062034
Stiles JC, Sparks W, Ronzio RA. The inhibition of Candida albicans by oregano. Journal of Applied Nutrition 1995;47:96-102.
Walker AF, Middleton RW, Petrowicz O. Artichoke leaf extract reduces symptoms of irritable bowel syndrome in a post-marketing surveillance study. Phytother Res. Feb 2001;15(1):58-61.
Whorwell PJ, Altringer L, Morel J, et al. Efficacy of an encapsulated probiotic Bifidobacterium infantis 35624 in women with irritable bowel syndrome. The American Journal of Gastroenterology 2006 Jul;101(7): 1581-1590.
Zhu L, Ma Y, Ye S, Shu Z. Acupuncture for Diarrhoea-Predominant Irritable Bowel Syndrome: A Network Meta-Analysis. Evidence-Based Complementary and Alternative Medicine. 2018/05/27 2018;2018:2890465. doi:10.1155/2018/2890465